

As code officials, our mission could be summarized as making sure all buildings are built in a manner where all occupants can rest assured that the building and its systems were constructed with their safety and wellbeing as a top priority. With that in mind, I’ve been researching, studying, and attempting to impact building safety in an area I’ve previously given little thought. You will understand what’s motivating me when I share a few statistics. The Centers for Medicare and Medicaid Services (CMS) have stated that nursing homes have been severely impacted by COVID-19, with outbreaks causing high rates of infection, morbidity, and mortality. The Centers for Disease Control and Prevention has stated that while data about infections in long-term care facilities (LTCFs) is limited, we do know that 1 to 3 million serious infections occur every year in these facilities. Infections are a major cause for hospitalizations and death; as many as 380,000 people die of infections in LTCFs every year. Available information as to deaths related to COVID-19 varies but suggests that deaths of residents of nursing homes (and similar facilities) may account for 25 to 42 percent of all COVID-19 deaths. Indications also show that when the virus occurs in nursing homes (and similar facilities), it is not uncommon that up to 50 percent of the facilities’ residents die after infection. I believe these are alarming statistics; as life safety professionals, they should grab our attention. For me, they have.
Following the onset of the COVID-19 pandemic, I became interested in researching the effects of air quality within nursing homes and similar facilities. The topic came to light when one of the nursing homes in Rockwall experienced the death of several residents. Our city began consulting with HVAC experts and mechanical engineers in a quest to determine what potential changes we might put forward that could help to protect the vulnerable occupants of facilities now and in the future.
As many of you may already be aware, the American Society of Heating, Refrigerating, and Air-Conditioning Engineers (ASHRAE) Standard 170 Ventilation of Health Care Facilities should be applied to some of these facilities. If you’re wondering what buildings are required to comply with the standard, that’s a great question. Beginning with the 2015 International Mechanical Code (IMC), Section 407.1 states the following, “Mechanical ventilation for ambulatory care facilities and Group I-2 occupancies shall be designed and installed in accordance with this code and ASHRAE 170.” The International Building Code (IBC), Section 308.4, Institutional Group I-2 states the following, “Institutional Group I-2 occupancy shall include buildings and structures used for medical care on a 24-hour basis for more than five persons who are incapable of self-preservation. This group shall include, but not be limited to, the following: Foster care facilities, detoxification facilities, hospitals, nursing homes and psychiatric hospitals.”
Therefore, if your city has adopted the 2015 or 2018 IMC, you should be paying close attention to this requirement. I conducted a limited survey of cities within the Dallas-Fort Worth area and found that several responding cities were not fully aware that they should be enforcing the ASHRAE standard. While I cannot conclusively quantify the impact it has on the safety of building occupants, I have found evidence to indicate that when the standard has been met, the health and safety of building occupants is enhanced. I’ve been in communication with the Texas Health and Human Services (HHS) representatives in both the architectural and policy and rules units, and at their prompting, I submitted an open records request for HHS data relative to all LTCFs in Texas. I’m currently in the process of studying that data, on a quest to determine whether those statistics indicate or perhaps prove that the LTCFs that were built in conformance to ASHRAE Standard 170 have experienced less incidence of COVID-19 related infections, morbidity, and mortalities. The following table represents those statistics.
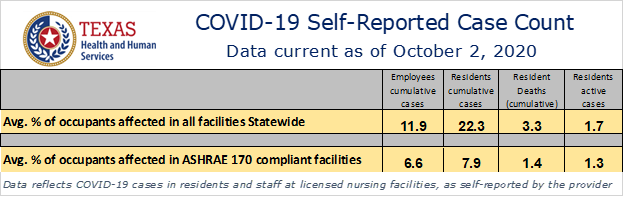
Based on these findings, it appears evident that facilities built in compliance with ASHRAE Standard 170 have experienced far less cases and deaths. I must point out, however, that statistically speaking, the sampling for available data relative to the compliant facilities is fairly small. The reason is because the State and HHS did not adopt or begin requiring conformance to ASHRAE Standard 170 until 2016. Therefore, the data available from HHS on facilities they know met the standard only includes the last four years. In addition, the vast majority of facilities licensed by HHS are assisted living or other type of LTCFs, and because HHS does not classify them as nursing facilities, they do not require them to comply with the ASHRAE standard. I must point out, there are other contributing factors which may influence and affect the prevention and/or spread of infections in these facilities. Operational practices most likely vary to a considerable degree from one facility to the next. The prudent care, or lack of care given during those practices, no doubt has an impact of the statistics I’ve provided. Unfortunately, I have no way to quantify that impact. It seems very reasonable, however, that we can surmise that conformance to two of the standards requirements alone, upgraded air changes per hour and enhanced filtration systems, will improve air quality and, therefore, occupant safety.
As code officials, we are not the only ones responsible to enforce ASHRAE Standard 170. HHS also works to regulate the air quality in these facilities. The State of Texas adopted ASHRAE 170 as a requirement on July 5, 2016. HHS is responsible for the licensing of nursing and assisted living homes constructed in Texas. When ASHRAE 170 applies to certain facilities, HHS will work to ensure through a permit, plan review, and on-site inspection process that the standard has been met prior to giving their approval for occupancy. In addition, the CMS adopted the National Fire Protection Association (NFPA) 99 Health Care Facilities Code in May 2016, which also contains reference to and requirements that ASHRAE Standard 170 be met.
If you haven’t already done so, I strongly encourage you to take some time and review the ASHRAE 170. It’s really not that complicated. One good option to confirm a new building will be constructed in compliance would be to require the mechanical engineer to specifically note on his submitted building plans, that the ventilation system was designed in conformance with the standard. Additionally, you could require the engineer to provide you with a letter prior to issuance of a C.O. that the system was built in conformance to his plans and complies with the standard.
If you come to the conclusion I have, that having this knowledge and ensuring any new facilities built in my city will be required to conform to the ASHRAE Standard 170, then I’m happy to know we will all be doing our part to enhance life safety, especially for the vulnerable occupants within our nursing facilities.
Jeffrey Widmer, CBO
President, BOAT
Building Official, City of Rockwall